




Dry eye, also known as keratoconjunctivitis sicca, is one of the most common eye conditions seen in community pharmacy. Dry eye is both gender and age-related. It generally tends to affect people above 60, and it is more common in women than men. Up to a third of people aged 65 or older may have dry eye. However, it is important to keep in mind that up to 30% of the population will experience dry eye at some point in their lives.
Although dry eye is not usually a serious condition it should not be underestimated either due to its effect on a patient’s health and wellbeing. It is also important to keep in mind that in rare cases, if left untreated dry eye syndrome has caused visual impairment and scarring of the eye’s surface. This condition provides community pharmacists with an opportunity to offer advice and share expertise in the treatment and management of this condition.
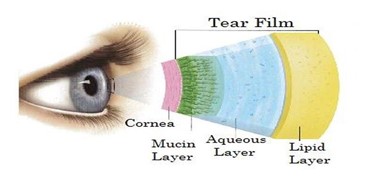
Figure 1: three layered tear film covering the epithelial layer of cornea
Tears serve several important functions:
Tears are produced and regulated by a system known as the lacrimal functional unit which consist of lacrimal gland, meibomian glands, eyelid, cornea and tear ducts. If any part of the lacrimal functional unit is interrupted the system can break down, resulting in the quantity (low aqueous flow) and or the quality (excessive tear film evaporation) of the tears being affected. This in turn causes tear hyperosmolarity which causes damage to the surface epithelium of the eye by activating a cascade of inflammatory events at the ocular surface and a release of inflammatory mediators into the tears. Epithelial damage involves cell death by apoptosis, a loss of goblet cells and disturbance of mucin expression leading to tear film instability. This instability exacerbates ocular surface hyperosmolarity and completes the vicious circle.
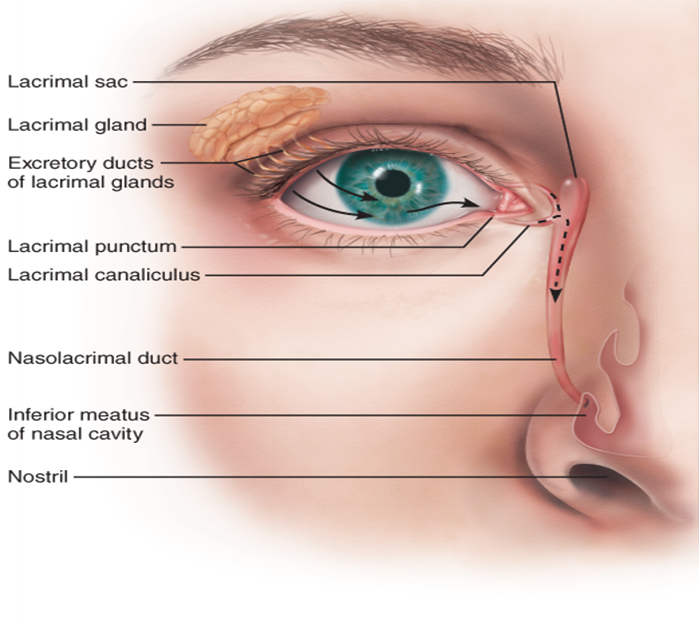
Figure 2: Lacrimal gland secretes lacrimal fluid onto the ocular surface
Environment: Factors such as sun, wind, dry climate, hot blowing air, high altitude can have a drying effect on the eyes. Regular exposure to these environmental factors can cause dry eye syndrome. For example, the combination of dry climate and warm air conditioning found in many offices can cause dry eye in some people.
Occupation: Activities that require visual concentration such as computer work, reading and writing tend to reduce blinking leading to tear evaporation and dry eye.
Medicines: Many commonly prescribed medicines and OTC medicines can cause or exacerbate dry eye in some people. These include antihistamines, anti-cholinergics, anti-depressants, beta-blockers, diuretics, vasoconstrictive eye drops, oral contraceptives, retinoids, anti-arrhythmics.
Laser surgery: Some people after having LASIK surgery can experience dry eye in weeks after surgery. However, the symptoms generally clear up after a few months.
Contact Lenses: Contact lenses can irritate the eye and cause dry eye syndrome. Contact lens wearers are 12 times more likely than non-contact lens wearers to report dry eye symptoms. Changing to a different type of lens or limiting their use, usually helps to resolve the symptoms.
Other possible causes of dry eye:
If any of the following present, immediate referral is advised:

Figure 3: Location of the Meibomian glands

The aim of treatment is to relieve the symptoms associated with dry eye, return the ocular surface and tear film to its normal homeostatic state, and prevent or minimise possible structural damage to the ocular surface. Although symptoms are rarely eliminated, they can often be improved with treatment.
When choosing a lubricant, it is important to take into consideration certain factors to ensure the best patient compliance:
Does blurring of vision occur after application and for how long: Gels have less blurring effect than ointments;
Duration and frequency of use: Gels have longer retention times than solutions;
Preservatives added to prevent bacterial growth in lubricants. Frequent use of preservative drops can cause irritation. If irritation occurs, preservative free formulations are more appropriate for user. Ideally a preservative that completely dissipates before reaching the tear film is best. Ointments generally do not support bacterial growth and do not require preservatives;
Once opened, how long does the product last: 28 days, 3 months, or 6 months; and
| Key question: Are the eyes dry due to aqueous deficiency or excessive evaporation? | |||
| Features of aqueous deficiency: Unable to produce tears when crying Sore eyes on waking without a history of recent eye injury Pain | Features of evaporative deficiency: Excessive watering on windy day Blepharitis Ocular Rosacea | ||
| Aqueous deficiency | Evaporative deficiency | ||
| Mild (<4 drops a day) | Moderate (4-6 drops a day) | Severe (>6 drops a day) | Systane Propylene glycol 0.6% eye drops preservative free |
| Hypromellose 0.5% eye drops | Hypromellose 0.3% eye drops, preservative free | Carmellose 0.5% eye drops, preservative free | Systane Balance Propylene glycol 0.6% eye drops |
| Polyvinyl alcohol 1.4% eye drops | Sodium hyaluronate 0.2% eye drops preservative free | Thealoz Duo (Sodium hyaluronate 0.15% & trehalose 0.3% drops) preservative free | Advice on lid hygiene |
| Carbomer 0.2% eye gel | Other options may be recommended in secondary care (VisuXL, Ikervis) | ||
| Finding an effective treatment can vary between patients. Try at least two products prior to stepping up to next level of treatment | |||
| At night in both aqueous and evaporative deficiency: Paraffin eye ointment preservative free Carbomer 0.2% eye gel | Note: preservative free preparations should be used in the following situations: Patients with ocular surface eye disease Patients with contact dermatitis to preservatives in eye products Soft contact lens wearers Patients with evidence of punctuate epithelial erosion from use of preservatives Frequency more than 6 times daily or using multiple preserved preparations | ||
Taking into consideration the significant percentage of people in the general population that suffer with dry eye and the fact that community pharmacy serves an older population, pharmacists can play an important role in supporting patients in the management and treatment of dry eye:
References available on request



